What Are The Major Causes Of Heel Painfulness
Overview
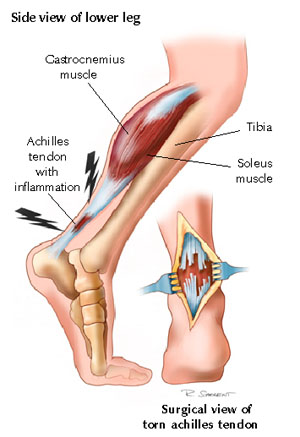
Every time you take a step, one of your heels has to support the whole weight of your body. As you move, the load is equal to 20 times your own body weight. The load is softened by a pillow of fat under the heel and a large sinew or ligament (the fibrous tissue that joins muscle and bone together) under the sole of the foot. This sinew is called the plantar fascia and it pulls the heel bone forward (in opposition to the Achilles tendon, which pulls it backwards). If an athlete does not warm up properly or a person with a sedentary job exercises heavily during the weekends, they might overload the muscles of the calf or strain the Achilles tendon, which joins these muscles to the heel bone. When overloaded the tendon becomes tight and painfully inflamed, which places extra strain on the plantar fascia and muscles in the soles of the foot. The strained plantar fascia becomes inflamed and may even develop tiny cracks. This is known as plantar fasciitis. Every time you sit down, sleep or otherwise rest your legs, the muscles of the sole of the foot will contract in an attempt to protect the damaged sinew. The pain in the heel will then no longer be felt. But when you get up again and put weight on the foot, the foot and ankle may feel stiff (because of the inflammation) and the pain will return either at the back of the heel or on the soles of the feet. When you start to move, the plantar fascia may crack even more causing a vicious cycle of damage and pain. Inflammation at the point where the Achilles tendon (at the back of the heel) or the plantar fascia (under the heel) join the heel bone (a bone known as the Calcaneum) stimulates cells that form bone to deposit bone in this area, eventually leading to the build up of a bony prominence on the heel bone called a calcaneal spur. But it's not the spur itself that causes the pain. The spur is a sign of chronic inflammation in the connective tissues, which is the result of a prolonged overload. It should also be pointed out that heel spurs can occur on their own, without plantar fasciitis or pain, or may be linked to some types of arthritis (inflammation of the joints). And plantar fasciitis or Achilles tendonitis don't necessarily lead to spur formation.
Causes
There are two different categories of heel pain. The first is caused by over-use repetitive stress which refers to a soreness resulting from too much impact on a specific area of the foot. This condition, often referred to as "heel pain syndrome," can be caused by shoes with heels that are too low, a thinned out fat pad in the heel area, or from a sudden increase in activity. Plantar fasciitis, a very common diagnosis of heel pain, is usually caused from a biomechancial problem, such as over-pronation (flat feet). The plantar fascia is a broad band of fibrous tissue that runs along the bottom surface of the foot, from the heel through the midfoot and into the forefoot. Over-pronation can cause the plantar fascia to be excessively stretched and inflamed, resulting in pain in the heel and arch areas of the foot. Often the pain will be most intense first thing in the morning or after a prolonged period of rest. The pain will gradually subside as the day progresses.
Symptoms
See your doctor as soon as possible if you experience severe pain accompanied by swelling near your heel. There is numbness or tingling in the heel, as well as pain and fever. There is pain in your heel as well as fever. You are unable to walk normally. You cannot bend your foot downwards. You cannot stand with the backs of the feet raised (you cannot rise onto your toes). You should arrange to see a doctor if the heel pain has persisted for more than one week. There is still heel pain when you are not standing or walking.
Diagnosis
Your doctor will perform a physical exam and ask questions about your medical history and symptoms, such as have you had this type of heel pain before? When did your pain begin? Do you have pain upon your first steps in the morning or after your first steps after rest? Is the pain dull and aching or sharp and stabbing? Is it worse after exercise? Is it worse when standing? Did you fall or twist your ankle recently? Are you a runner? If so, how far and how often do you run? Do you walk or stand for long periods of time? What kind of shoes do you wear? Do you have any other symptoms? Your doctor may order a foot x-ray. You may need to see a physical therapist to learn exercises to stretch and strengthen your foot. Your doctor may recommend a night splint to help stretch your foot. Surgery may be recommended in some cases.
Non Surgical Treatment
Physical medicine modalities are well known for their benefits and they have been consistently applied in early treatment of plantar fasciitis. Typically, the direct application of ice, ice baths or contrast soaking aid in the local reduction of inflammation and temporarily augment pain management. Electric stimulation may only provide indirect reduction of interstitial inflammation of the plantar fascia. Ultrasound therapy, hot pack systems and deep tissue massage help eliminate inflammation and aid in restoring plantar fascia tensegrity. Generally, these modalities are considered to be valuable adjuncts to a well-organised treatment plan. Various programs of stretching, range of motion and therapeutic exercises can help re-establish foot function and improve tolerance to load. When it is done appropriately, stretching can serve as an important adjunct to the resumption of the plantar fascia?s ability to tolerate eccentric loading forces that typically occur during stance and gait. Night splinting has proven to be an effective tool in managing persistent plantar fasciitis. Antiinflammatory modalities, such as ice and ice baths, are often the first line of treatment. Oral NSAIDs have been a mainstay of treatment. While they effectively relieve symptoms, be aware that they frequently fail to promote sustained relief. When inflammation is severe or fails to respond to initial efforts, one may consider corticosteroid injection(s). However, keep in mind that corticosteroid injections impose the risk of aponeurosis rupture secondary to focal collagen tissue necrosis and can result in focal heel fat pad atrophy.
Surgical Treatment
Surgery to correct heel pain is generally only recommended if orthotic treatment has failed. There are some exceptions to this course of treatment and it is up to you and your doctor to determine the most appropriate course of treatment. Following surgical treatment to correct heel pain the patient will generally have to continue the use of orthotics. The surgery does not correct the cause of the heel pain. The surgery will eliminate the pain but the process that caused the pain will continue without the use of orthotics. If orthotics have been prescribed prior to surgery they generally do not have to be remade.
heel pain pads
Prevention
Heel pain is commonly caused from shoes that do not fit properly. In addition, shoes need to have ample cushioning and support, particularly through the heel, ball of the foot, and arch. Shoes should also be replaced if they become too worn. One sure sign of wear and tear is overly worn areas of a shoe's insoles. If the heel or ball of the foot is particularly worn, damage could easily occur since the bottom of the foot is not getting the cushioning it needs.
Every time you take a step, one of your heels has to support the whole weight of your body. As you move, the load is equal to 20 times your own body weight. The load is softened by a pillow of fat under the heel and a large sinew or ligament (the fibrous tissue that joins muscle and bone together) under the sole of the foot. This sinew is called the plantar fascia and it pulls the heel bone forward (in opposition to the Achilles tendon, which pulls it backwards). If an athlete does not warm up properly or a person with a sedentary job exercises heavily during the weekends, they might overload the muscles of the calf or strain the Achilles tendon, which joins these muscles to the heel bone. When overloaded the tendon becomes tight and painfully inflamed, which places extra strain on the plantar fascia and muscles in the soles of the foot. The strained plantar fascia becomes inflamed and may even develop tiny cracks. This is known as plantar fasciitis. Every time you sit down, sleep or otherwise rest your legs, the muscles of the sole of the foot will contract in an attempt to protect the damaged sinew. The pain in the heel will then no longer be felt. But when you get up again and put weight on the foot, the foot and ankle may feel stiff (because of the inflammation) and the pain will return either at the back of the heel or on the soles of the feet. When you start to move, the plantar fascia may crack even more causing a vicious cycle of damage and pain. Inflammation at the point where the Achilles tendon (at the back of the heel) or the plantar fascia (under the heel) join the heel bone (a bone known as the Calcaneum) stimulates cells that form bone to deposit bone in this area, eventually leading to the build up of a bony prominence on the heel bone called a calcaneal spur. But it's not the spur itself that causes the pain. The spur is a sign of chronic inflammation in the connective tissues, which is the result of a prolonged overload. It should also be pointed out that heel spurs can occur on their own, without plantar fasciitis or pain, or may be linked to some types of arthritis (inflammation of the joints). And plantar fasciitis or Achilles tendonitis don't necessarily lead to spur formation.
Causes
There are two different categories of heel pain. The first is caused by over-use repetitive stress which refers to a soreness resulting from too much impact on a specific area of the foot. This condition, often referred to as "heel pain syndrome," can be caused by shoes with heels that are too low, a thinned out fat pad in the heel area, or from a sudden increase in activity. Plantar fasciitis, a very common diagnosis of heel pain, is usually caused from a biomechancial problem, such as over-pronation (flat feet). The plantar fascia is a broad band of fibrous tissue that runs along the bottom surface of the foot, from the heel through the midfoot and into the forefoot. Over-pronation can cause the plantar fascia to be excessively stretched and inflamed, resulting in pain in the heel and arch areas of the foot. Often the pain will be most intense first thing in the morning or after a prolonged period of rest. The pain will gradually subside as the day progresses.
Symptoms
See your doctor as soon as possible if you experience severe pain accompanied by swelling near your heel. There is numbness or tingling in the heel, as well as pain and fever. There is pain in your heel as well as fever. You are unable to walk normally. You cannot bend your foot downwards. You cannot stand with the backs of the feet raised (you cannot rise onto your toes). You should arrange to see a doctor if the heel pain has persisted for more than one week. There is still heel pain when you are not standing or walking.
Diagnosis
Your doctor will perform a physical exam and ask questions about your medical history and symptoms, such as have you had this type of heel pain before? When did your pain begin? Do you have pain upon your first steps in the morning or after your first steps after rest? Is the pain dull and aching or sharp and stabbing? Is it worse after exercise? Is it worse when standing? Did you fall or twist your ankle recently? Are you a runner? If so, how far and how often do you run? Do you walk or stand for long periods of time? What kind of shoes do you wear? Do you have any other symptoms? Your doctor may order a foot x-ray. You may need to see a physical therapist to learn exercises to stretch and strengthen your foot. Your doctor may recommend a night splint to help stretch your foot. Surgery may be recommended in some cases.
Non Surgical Treatment
Physical medicine modalities are well known for their benefits and they have been consistently applied in early treatment of plantar fasciitis. Typically, the direct application of ice, ice baths or contrast soaking aid in the local reduction of inflammation and temporarily augment pain management. Electric stimulation may only provide indirect reduction of interstitial inflammation of the plantar fascia. Ultrasound therapy, hot pack systems and deep tissue massage help eliminate inflammation and aid in restoring plantar fascia tensegrity. Generally, these modalities are considered to be valuable adjuncts to a well-organised treatment plan. Various programs of stretching, range of motion and therapeutic exercises can help re-establish foot function and improve tolerance to load. When it is done appropriately, stretching can serve as an important adjunct to the resumption of the plantar fascia?s ability to tolerate eccentric loading forces that typically occur during stance and gait. Night splinting has proven to be an effective tool in managing persistent plantar fasciitis. Antiinflammatory modalities, such as ice and ice baths, are often the first line of treatment. Oral NSAIDs have been a mainstay of treatment. While they effectively relieve symptoms, be aware that they frequently fail to promote sustained relief. When inflammation is severe or fails to respond to initial efforts, one may consider corticosteroid injection(s). However, keep in mind that corticosteroid injections impose the risk of aponeurosis rupture secondary to focal collagen tissue necrosis and can result in focal heel fat pad atrophy.
Surgical Treatment
Surgery to correct heel pain is generally only recommended if orthotic treatment has failed. There are some exceptions to this course of treatment and it is up to you and your doctor to determine the most appropriate course of treatment. Following surgical treatment to correct heel pain the patient will generally have to continue the use of orthotics. The surgery does not correct the cause of the heel pain. The surgery will eliminate the pain but the process that caused the pain will continue without the use of orthotics. If orthotics have been prescribed prior to surgery they generally do not have to be remade.
heel pain pads
Prevention
Heel pain is commonly caused from shoes that do not fit properly. In addition, shoes need to have ample cushioning and support, particularly through the heel, ball of the foot, and arch. Shoes should also be replaced if they become too worn. One sure sign of wear and tear is overly worn areas of a shoe's insoles. If the heel or ball of the foot is particularly worn, damage could easily occur since the bottom of the foot is not getting the cushioning it needs.